Anyone who is paying attention to the cannabis industry knows that our knowledge about cannabis science is growing rapidly. There has never been a more exciting time for cannabis enthusiasts and scientists, as new products and information are coming out weekly. New cannabinoid homologues (molecules with similar-but-different structural features) continue to be found even today, over 100 years after the first cannabinoid was discovered.
Despite continued discoveries in recent years about cannabis, some of the cannabinoid discoveries from the past are still very pertinent today and still have not been fully explored. One example of this is tetrahydrocannabivarin (THCV), which is a unique cannabinoid that was first discovered 50 years ago, but scientists are still studying how to best utilize it.1
Tetrahydrocannabivarin is structurally very similar to the best-known cannabinoid: tetrahydrocannabinol (THC). In fact, the difference between these two molecules is only two carbons. THCV is nearly identical to THC, but with a shorter carbon tail–a nominal difference in overall appearance. This tail, however, is an extremely important contributor to the effects of cannabinoids; it’s known as the pharmacophore and changing its size can change the way the drug acts on the CB receptors (and others).2
What’s most exciting about THCV is its promise in treating obesity and diabetes. This is mostly due to its ability to block activation of the CB1 receptors, which is the receptor responsible for triggering the munchies after THC ingestion. In a high quality, randomized, placebo-controlled trial, THCV was able to improve the fasting blood glucose levels among type II diabetics.7 Additionally, multiple animal models have suggested that THCV could be useful for combating addiction, nicotine in particular.8 Lastly, THCV may also be able to produce neuroprotective effects in brain injuries, as well as neurodegenerative disease.5 Unfortunately there is still plenty of science to be done to really harness the benefits of THCV and for now there are not many products.
As mentioned, the only difference between THC and THCV is the length of their tails. With a 3-carbon tail (-propyl) rather than a 5-carbon tail(-pentyl), it is thought that THCV can have very different effects in the body than THC. Though, THCV does indeed interact with CB1 and CB2, so there could be intoxicating and immunomodulatory effects from this cannabinoid similar to those of THC.
THCV’s actions can vary depending on the dose. At doses around 5x higher, THCV can be similar to THC, interacting with CB1 and causing hallmark effects of THC including intoxication, analgesia, and hypothermia. These effects come as little surprise, given the similarities to THC, however, lower doses of THCV may function as an antagonist of CB1. This means that THCV would act by competing with THC or endocannabinoids at the CB1 receptor. Blocking this receptor is a known treatment for obesity and metabolic syndrome, as shown through high-quality studies on rimonabant, a selective CB1 antagonist that was approved in 2006 in the EU. Rimonabant’s time on the market was short lived; it was withdrawn within a couple years, due to increased risk of mood problems, depression, and anxiety.11 It is thought that these side effects were secondary to blocking the action on endocannabinoids. Because THCV does not engage the CB receptors as aggressively as rimonabant, it may be possible to use it to block some actions of CB1, but without causing the major side effects of the pharmaceutical product, rimonabant.
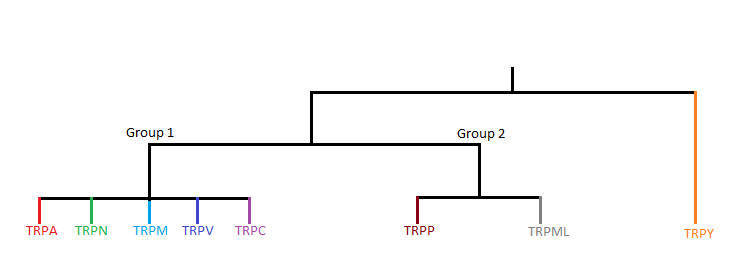
But THCV’s activity does not stop with the classical receptors CB1 and CB2. In fact, some data suggests that while the shorter side chain detracts from CB1 and CB2 affinity, it increases the affinity for the TRPA1 channel. This difference in affinity could help explain the differences noted between the effects of THCV and THC, but the clinical meaning of this is still unclear.4
THCV may have other neuroprotective effects beyond the CB1 and CB2 receptors. There is speculation that some THCV’s net effects could be mediated through a nuclear receptor known as PPAR-gamma, especially the effects seen in diabetic patients. Additionally, THCV appears to penetrate the CNS well, making it a desirable candidate for treating neurological disease.4,5
If one looks at the current legal cannabis market, one will quickly notice there are few products available that are high in THCV. The primary reason these products are hard to find is because THCV is a relatively rare cannabinoid. The limited science we have suggests the homologue is more common in Indica (wide-leaf) varieties, while less common in sativa varieties (narrow-leaf) of the plant.6 Even the few cannabis chemovars (strains) that do produce THCV, they often do so in small amounts. And even when they do produce, they almost always do so alongside THC. In other words, if you find a THCV-dominant product on the market, it is likely a result of a process known as distillation or isolation, not a direct expression of the cannabinoid profile of the plant from which it was extracted. If breeders want naturally high THCV strains, they have many years of work ahead of them to develop stable genetics that produce this short-tailed homologue.
While THCV shows promise in the treatment of several conditions and may prove to be pharmacologically important, let’s not forget the ever-growing number of minor cannabinoids that may hold therapeutic benefits. Scientists recently confirmed the existence of a long-tailed (7-carbon) homologue known as THCP, but its pharmacologic significance remains questionable, at least in natural amounts.9 Other cannabinoid homologues continue to be discovered each year, and we have begun to learn they are somewhat common in many cannabis varieties.10 Each of these cannabinoids have similar but different pharmacologic features and each could have major impacts on cannabinoid therapeutics in the future.
Go to trichomes.com to see this article.
1 Merkus FW. Cannabivarin and tetrahydrocannabivarin, two new constituents of hashish. Nature. 1971;232(5312):579-580. doi:10.1038/232579a0
2 Bow EW, Rimoldi JM. The Structure-Function Relationships of Classical Cannabinoids: CB1/CB2 Modulation. Perspect Medicin Chem. 2016;8:17-39. Published 2016 Jun 28. doi:10.4137/PMC.S32171
3 Tudge L, Williams C, Cowen PJ, McCabe C. Neural effects of cannabinoid CB1 neutral antagonist tetrahydrocannabivarin on food reward and aversion in healthy volunteers. Int J Neuropsychopharmacol. 2014;18(6):pyu094. Published 2014 Dec 25. doi:10.1093/ijnp/pyu094
4 Pertwee RG. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br J Pharmacol. 2008;153(2):199-215. doi:10.1038/sj.bjp.0707442
5 Stone NL, Murphy AJ, England TJ, O’Sullivan SE. A systematic review of minor phytocannabinoids with promising neuroprotective potential. Br J Pharmacol. 2020;177(19):4330-4352. doi:10.1111/bph.15185
6 Hillig KW, Mahlberg PG. A chemotaxonomic analysis of cannabinoid variation in Cannabis (Cannabaceae). Am J Bot. 2004;91(6):966-975. doi:10.3732/ajb.91.6.966
7 Jadoon KA, Ratcliffe SH, Barrett DA, et al. Efficacy and Safety of Cannabidiol and Tetrahydrocannabivarin on Glycemic and Lipid Parameters in Patients With Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled, Parallel Group Pilot Study. Diabetes Care. 2016;39(10):1777-1786. doi:10.2337/dc16-0650
8 Xi ZX, Muldoon P, Wang XF, et al. Δ8 -Tetrahydrocannabivarin has potent anti-nicotine effects in several rodent models of nicotine dependence. Br J Pharmacol. 2019;176(24):4773-4784. doi:10.1111/bph.14844
9 Citti, C., Linciano, P., Russo, F. et al. A novel phytocannabinoid isolated from Cannabis sativa L. with an in vivo cannabimimetic activity higher than Δ9-tetrahydrocannabinol: Δ9-Tetrahydrocannabiphorol. Sci Rep 9, 20335 (2019). https://doi.org/10.1038/s41598-019-56785-1
10 Bueno, J. Greenbaum, EA. (−)-trans-Δ9-Tetrahydrocannabiphorol Content of Cannabis sativa Inflorescence from Various Chemotypes. Journal of Natural Products 2021 84 (2), 531-536 DOI: 10.1021/acs.jnatprod.0c01034
11 Sam AH, Salem V, Ghatei MA. Rimonabant: From RIO to Ban. J Obes. 2011;2011:432607. doi:10.1155/2011/432607



{kind=link}
{kind=link}